

INTRODUCTION
Saturation of acid-etched enamel axial surfaces with liquid-free resin to inhibit the progress of decalcification early in the caries process is not new. Regardless of whether phosphoric or hydrochloric acid has been used for etching, this method has been called “micro-restorative dentistry”, “smooth surface sealer application” and “resin impregnation”. DMG currently uses the term “resin filtration” for its product, Icon.1-8
After treating adolescents in private practice for many years, it has been observed that the back teeth are often foreign to toothbrushing and flossing in such patients. Some teenagers brush the teeth they see in the mirror when they smile and neglect the ones in the back of the mouth. The buccal surfaces of the first and second molars are often seen with plaque build-up and the resulting decalcification and caries lesions, but other axial surfaces are also susceptible.
Two examples of adolescents with lesions of the oral surface are depicted. In November 2006, the first patient was shown to have a significant Class V cavitary caries lesion requiring a resin-modified glass ionomer restoration. The restored tooth was photographed in August 2019. The other patient not only had occlusal carious grooves that required preventive resin repair9 but also decalcification of the oral surface, which was treated by modification of the “smooth surface sealer” using Adper Prompt L Pop (3M) and ACTIVA BioACTIVE-RETORATIVE (Pulpdent).2.3 With a pictorial essay, treatments for affected oral surfaces are presented (Figures 1 to 15).
DISCUSSION
Vitremer resin-modified glass ionomer (3M) was chosen to restore the oral surface in the first patient for several reasons: the material’s fluoride content, the material’s coefficient of thermal expansion similar to that of tooth structure resulting in excellent marginal integrity . time and the resin component that makes such materials more resistant to abrasion from tooth brushing and corrosion from the acidic oral environment. Furthermore, this material was convincingly demonstrated in a retrospective study of hundreds of primary tooth restorations.10
The decalcification treatment in the second case was a modification of the “smooth surface sealer”.2.3 Instead of painting the etched surface with only unfilled resin binder, the cured adhesive was covered with a thin layer of ACTIVA Bio-ACTIVE material. This gives a slightly thicker cemented coating containing fluoride for the surface, which would reasonably protect against the wear and tear of tooth brushing and renewed decalcification. The fluoride, calcium and phosphate content in ACTIVA could possibly have a positive effect on the enamel involved. The use of an unfilled bonding agent prior to placement of a resin adhesive sealant has been shown to be effective in treating cavities and fissures.13,14 The full value of bonding one type of resin-filled material to create a “reinforced” smooth surface sealer, as shown here, would make a worthwhile in vitro study in an artificial caries model.
PATIENT FIRST
Figure 1. A 17-year-old patient with plaque accumulation on the maxillary second molar.
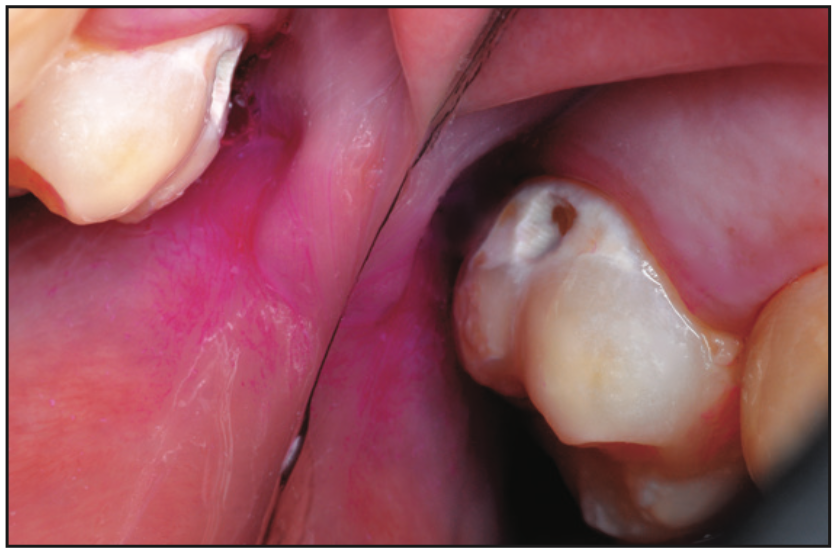
Figure 2. Scraping of the cleoid through the calcification revealed the cavitation.

Figure 3. After local anesthetic injection, low speed preparation was done with round burrs. Mechanical restraint using a slow-speed inverted taper increased glass ionomer bonding.
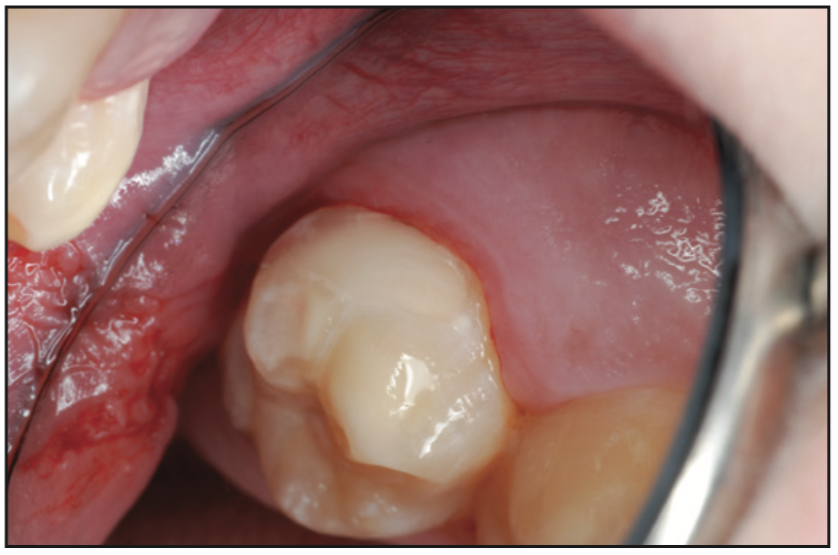
Figure 4. Vitremer10 resin-modified glass ionomer material was injected, lightly cured, shaped, finished, and polished.

Figure 5. Resin-modified glass ionomer repair seen at 12 years, 10 months postoperatively, before dental cleaning.
PATIENT TWO
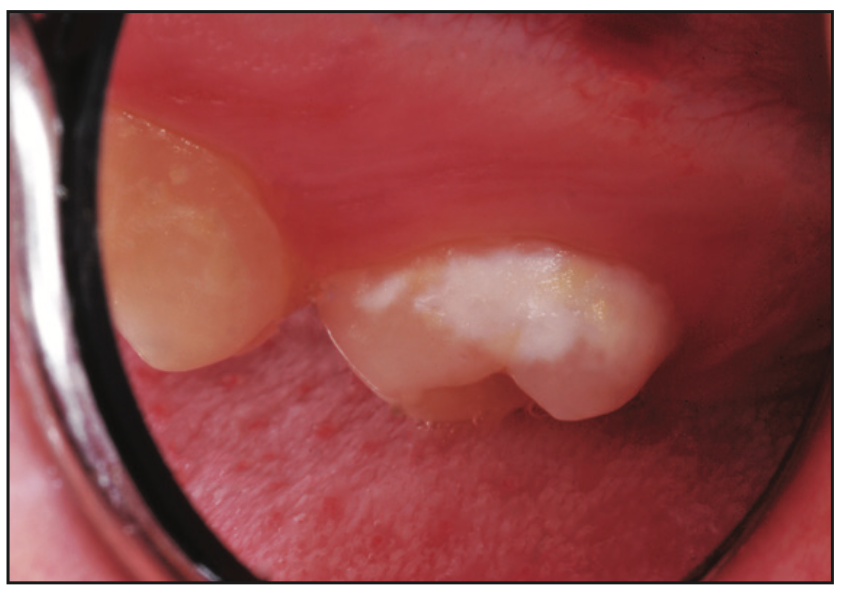
Figure 6. Decalcification of the second molar oral surface in a 15-year-old patient.
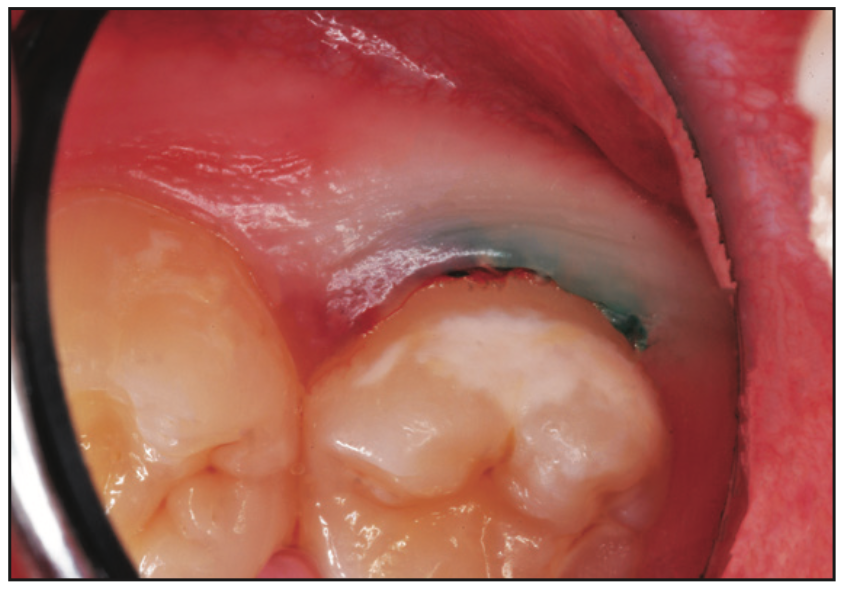
Figure 7. After local anesthesia with infiltration, a retraction cord was placed.
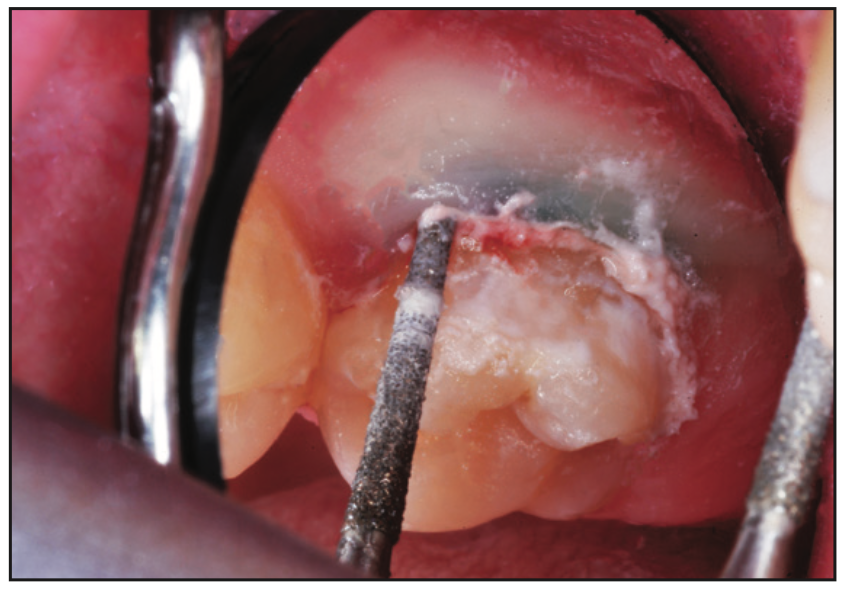
Figure 8. The decalcified enamel was cut smooth with a slow speed diamond.
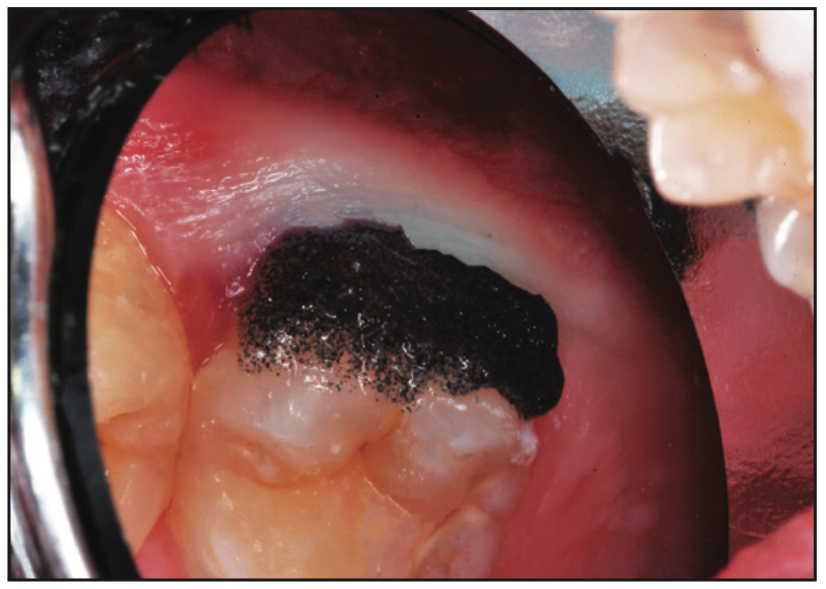
Figure 9. A 40% phosphoric acid (Onyx LG [Centrix]) was applied for 30 seconds.
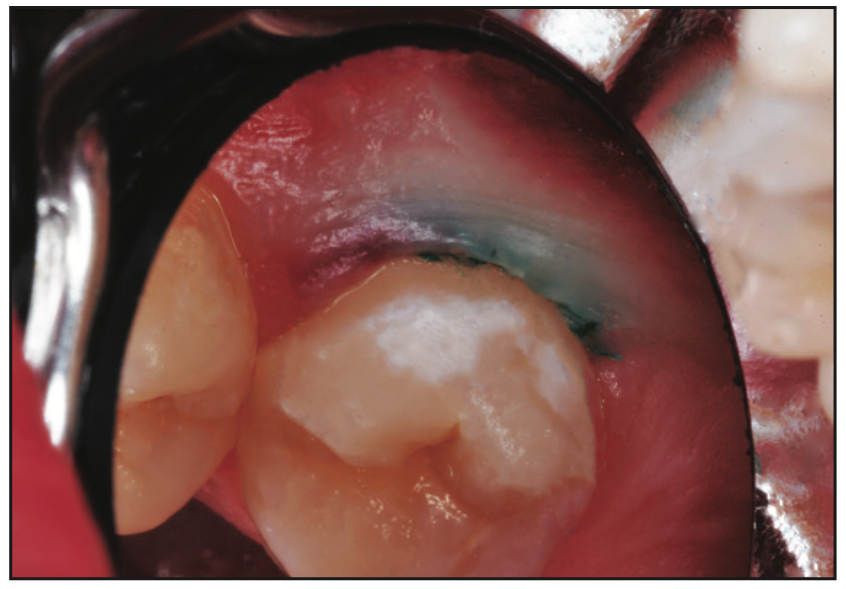
Figure 10. The surface was rinsed and dried with a water/air spray. Some white decalcified enamel remained, but the surface was scratch resistant.
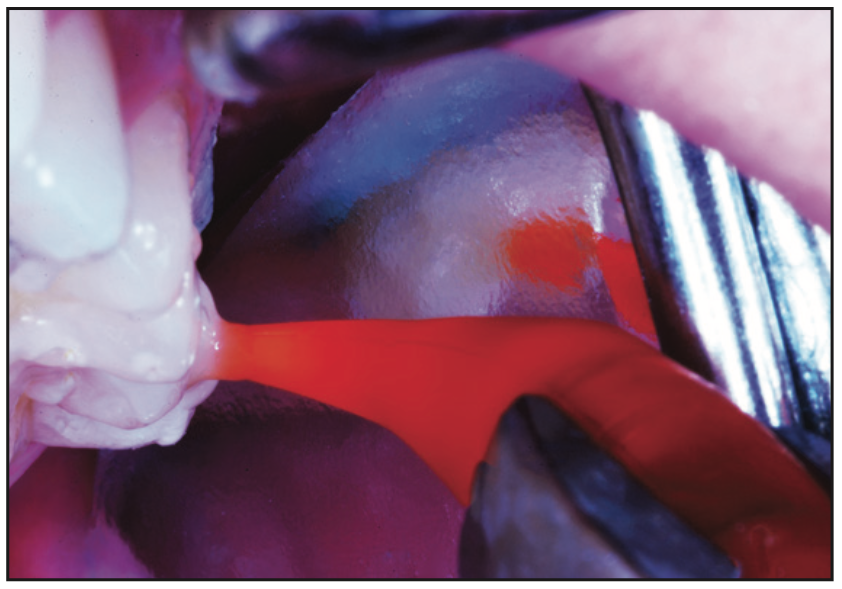
Figure 11. After unfilled resin binder (Adper Prompt L Pop [3M]) was applied to the surface and light-cured, ACTIVA BioACTIVE-RETORATIVE (Pulpdent), shade A1, was injected and spread in a thin layer with the side of an explorer #23.11,12
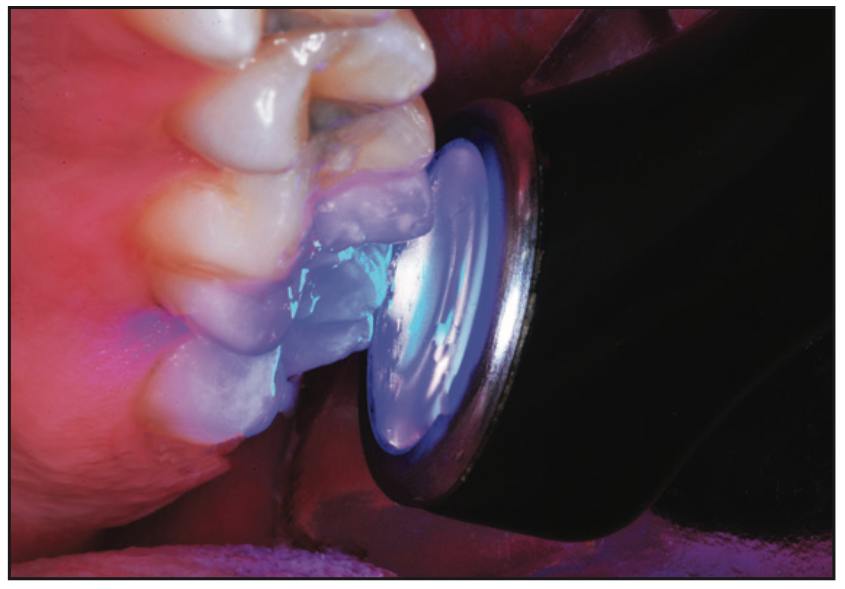
Figure 12. The ACTIVA-coated surface was exposed to a curing light beam (1,100 mW/cm2) for 20 seconds.
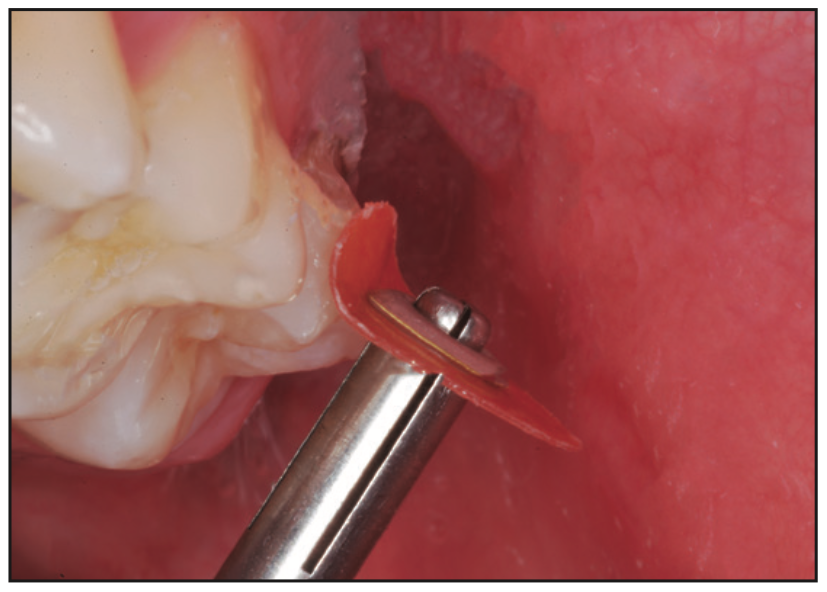
Figure 13. The surface was finished and polished smooth with a series of aluminum oxide discs (Sof-Lex [3M]).
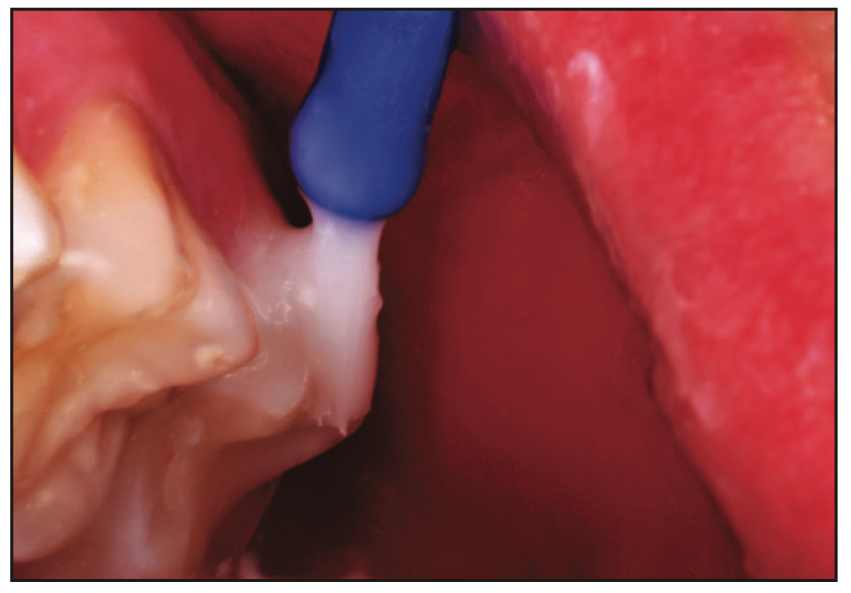
Figure 14. After preventive resin restoration of the occlusal grooves, the entire crown was painted with 5% fluoride varnish.9
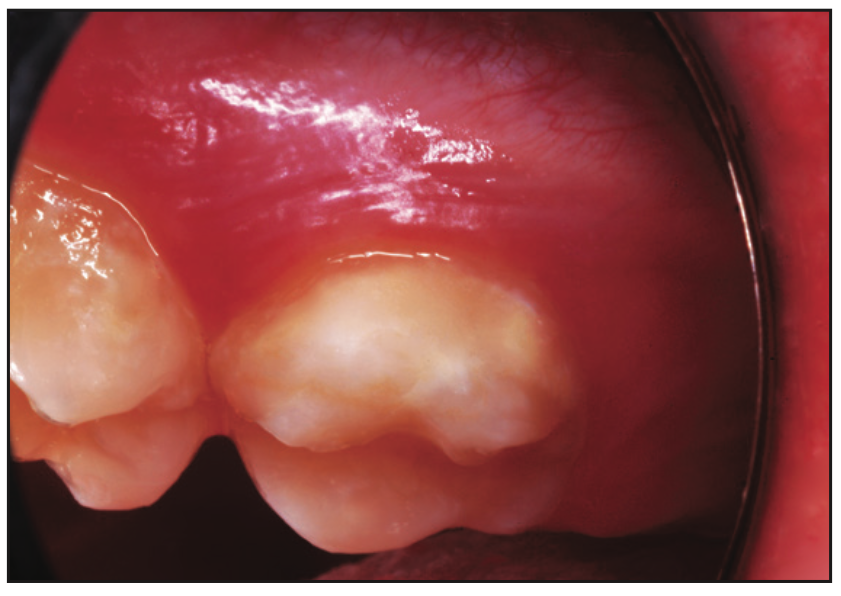
Figure 15. Buccal surface seen 9 months after application of the “reinforced” smooth surface sealer. The A1 shade of ACTIVA appears whiter than the oral enamel.
BIBLIOGRAPHICAL REFERENCES
1. Robinson C, Hallsworth AS, Weatherell JA, et al. Arrest and control of carious lesions: a study based on preliminary experiments with resorcinol-formaldehyde resin. J Dent Res. 1976, 55(5):812–8. doi:10.1177/00220345760550051601
2. TP rotation. Bonded resin sealant for smooth surface enamel defects: new concepts in “micro-restorative” dentistry. Quintessence Int. 1987, 18(1):5-10.
3. TP rotation. Restorative dentistry for preschool children: Smooth surface sealants. In: Johnson D, Tinanoff N, eds. Dental Clinics of North America: Dental Care for the Preschool Child. WB Saunders; 1995:39(4):745.
4. Glasspoole EA, Erickson RL, Davidson CL. Protective effects of resin impregnation on enamel desalination. Am J Dent. 1999, 12(6):315–20.
5. Paris S, Meyer-Lueckel H, Kielbassa AM. Resin infiltration of natural caries lesions. J Dent Res. 2007;86(7):662–6. doi:10.1177/154405910708600715
6. Paris S, Meyer-Lueckel H. Concealment of labial enamel white spot lesions with resin infiltration – a clinical report. Quintessence Int. 2009? 40 (9): 713–8.
7. Torres CR, Borges AB. Color coverage of developmental enamel defects: a case series. Opera Dent. 2015? 40 (1): 25-33. Doi:10.2341/13-346-T
8. Nizami N, Lawson N. Treatment of white spot lesions with resin infiltration. Dent Today. 2021? 40 (8): 90–3.
9. Simonsen RJ. Chapter 8: Preventive resin restorations. In: Simonsen RJ, ed. Clinical Applications of the Acid Etch Technique. Quintessence Publishing; 1978:89-95.
10. Croll TP, Bar-Zion Y, Segura A, et al. Clinical performance of resin-modified glass ionomer cement restorations in primary teeth. A retrospective evaluation. J Am Dent Assoc. 2001? 132(8):1110-
6. Doi:10.14219/jada.archive.2001.0336
11. Croll TP, Berg JH, Donly KJ. Dental repair material: a resin-based bioactive ionic glass-ionomer modified composite. Compend Contin Educ Dent. 2015? 36 (1): 60–5.
12. Croll TP, Lawson NC. Repair of bonded Class I and Class II teeth with resin-based bioactive ionic glass ionomer modified composite. Dent Today. 2020? 39(1):86–9.
13. Croll TP. The quintessential sealant? Quintessence Int. 1996;27(11):729-32.
14. Feigal RJ, Musherure P, Gillespie B, et al. Improved sealant retention with adhesives: a clinical study of two-bottle and one-bottle systems. J Dent Res. 2000;79(11):1850–6. Doi: 10.1177/00220345000790110601
ABOUT THE AUTHORS
Dr. Kroll is the clinic director of Cavity Busters Doylestown in Doylestown, Pa. Assistant Professor of Pediatric Dentistry at the University of Texas Health Science Center at San Antonio School of Dentistry. and clinical professor of pediatric dentistry at Case Western Reserve School of Dental Medicine in Cleveland. He can be reached at willipus@comcast.net.
Dr. Bressler is president of Doc Bresler’s Cavity Busters, medical director at Red Lion Surgicenter, assistant professor of pediatric dentistry at Temple University Kornberg School of Dentistry, and assistant professor of pediatric dentistry at the University of Pennsylvania School of Dental Medicine. He can be reached at drbresler@hotmail.com.
Dr. Ferretti is professor and chair of pediatric dentistry at Case Western Reserve School of Dental Medicine and chief of dentistry at Rainbow Babies and Children’s Hospital at the Irving & Jeanne Tapper Pediatric Dental Center in Cleveland. He can be reached at gaf10@case.edu.
Disclosure: The authors report no disclosures.