

Gina Vega presents a clinical case that addressed patient crowding and shadow concerns through a combination of Invisalign clear aligner treatment and teeth whitening.
Patient details and concerns
A 42-year-old gentleman originally from Scotland had been working in London for the past eight years as a risk assessment consultant.
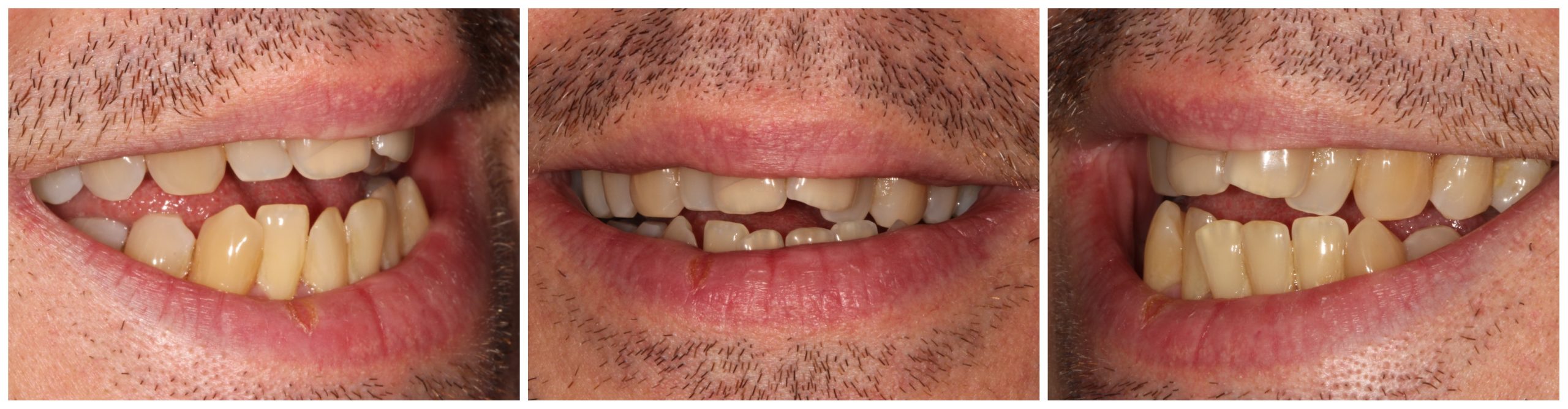
Rating his teeth a four out of 10, the patient was always very self-conscious. He felt unattractive with damaged self-esteem. He hid his teeth when he smiled for photographs and avoided social events with new people.
His main concern was overall crowding, especially in his two front teeth, which were so far forward that it looked like he had no teeth in the back.
His teeth were very dark and he wanted to make them whiter.
The patient had localized mild periodontitis and generalized gingivitis. Dental treatment was needed before any cosmetic treatment could begin. This should include visits to the hygienist to treat periodontal disease and advice on oral hygiene.

Alternative cure
The following options were discussed:
- No cure, acceptance of current situation
- Orthodontic treatment with Invisalign with L8s extractions
- Extraction-free Invisalign orthodontic treatment with extended interproximal reduction (IPR)
- Specific orthodontic referral that could be addressed with fixed braces, lingual braces, or clear aligners with possible advice for L4 or L8 extractions
- Teeth whitening after orthodontic treatment.
The patient was not looking to have a fixed retainer as he believed it would make him even more self-conscious about his smile and uncomfortable at work.
After considering his options, the patient consented to Invisalign without extractions and teeth whitening.
Download files
- Clinical photos
- iTero scan
- Orthopantography (OPG).
Radiographic report
Panoramic radiograph showed permanent adult dentition with multiple restorations.
There was mild generalized bone loss of approximately 10% in the molar regions. Root morphology was within normal limits.
Clinical
The patient presented skeletal class III, high FMPA without asymmetries and increased lower facial height. His lips were fit and modest. Intraoral examination revealed a class III right and left canine and a class I molar.
The patient’s overjet was 3mm and his overbite was reduced presenting an anterior open bite. Its upper and lower midline were centered with the lower slope to the right.
Moderate crowding was present in the upper and lower regions, with arch size deviation. A narrow upper arch presented with an irregular narrow buccal passage and prominent U1 and wider lower arch.
List of problems:
- Abnormal, narrow buccal passage
- Division of Class II Sectors 1
- Crowding of upper and lower arches
- Left cross bite
- Right contour for contour bite.
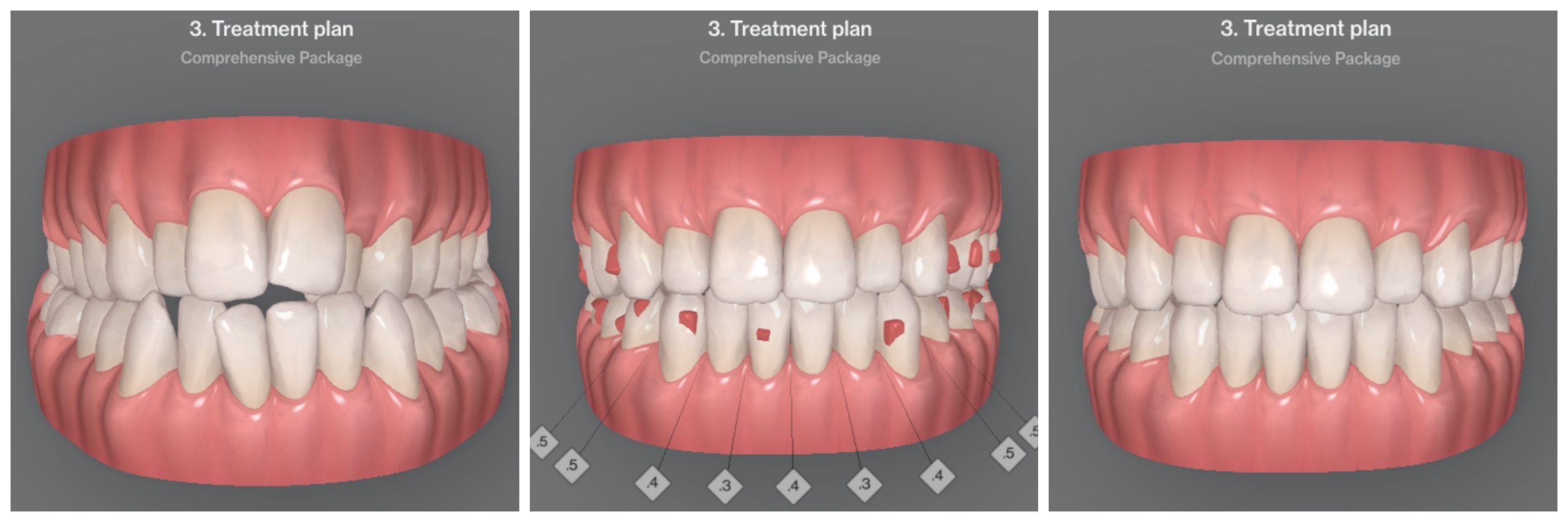
treatment plan
Invisalign Comprehensive with the following treatment goals:
- Expand the oral passageway
- Local class III to class I
- Resolve upper and lower arch crowding
- Fix general misalignment
- Increase the overbite.
A treatment plan involving L8 extractions was discussed with the patient at the first session, but the patient declined this option.
Protocols and case design
Prescription for Invisalign
- Please extend the upper arch into a parabolic arch, compressing distally to 7s
- When expanding, apply G8 protocols
- Oral and palatal edges to be flush with the occlusal plane on the upper and lower molars
- The occlusive plane should be symmetrical on the right and left sides
- Place horizontal 4 mm palatal oblique attachments on the upper anterior incisors
- Above 6s passive horizontal beveled components 5mm
- Bottom 6s passive horizontal bevel attachments 5mm
- Anterior to lower arch – start with crown torque to resolve crowding by intrusion and pronation (rotation) once contact points are in correct position add 0.2mm IPR between all incisors going from mid LR3 to mid LL3
- Complete the backstroke and add some lingual root torque, all in one go
- Align teeth with incisors.
Application of the recipe
Once I received the first Clincheck I use the 3D controls to implement my protocols. I always draw the upper arch first to have a symmetrical parabolic shape. When expanding, I make sure G8 protocols are implemented. This is the addition of buccal root torque to the molars to prevent buccal tipping of the crown as much as possible, but instead to allow actual physical movement of the molars.
In this case, the arch needed to be extended several millimeters, mainly to correct the border-to-border bite on the right and the crossbite on the left. It was also of utmost importance to give back symmetry to the buccal corridor and create the space required for retrograde U1s.
I used U8s as anchors to control the several millimeters of expansion and recoil I planned for the front end.
I placed passive attachments on 6 to aid anchorage and conventional orthogonal palatal attachments on the upper incisors to aid tooth movement.
Once the upper arch was drawn, I drew the lower arch, in this case starting with compression of the arch to help resolve the crossbite.
To solve the lower crowding IPR was added to the rear and front.
When invading the anterior segment, I request that both retraction and lingual torque of the root be applied at the same time. This helps physical movements in the bones and prevents receding gums.
After a series of modifications, Clincheck was approved with 27 upper and lower active aligners.
Attachments:
- Optimized UR7 and LL7 multi-level components
- Optimized upper and lower 3s, LR5, UL4, LL4 and LL5 rotation components
- Optimized LR4 root checker
- Optimized LR1 extrusion
- Optimized UR5 retainer
- Horizontal beveled fittings 5mm U6s
- 4mm horizontal beveled components on the palatal surface of U1s and U2s
- L6s horizontal occlusal bevel attachments.
The patient was re-examined every six to eight weeks.

Additional aligners
After alignment 27 it was noted that the upper arch needed further extension and alignment. The blockage also needed fixing. All attachments were removed before taking photos and a new iTero scan.
After a series of modifications, a new Clincheck was approved with 14 upper and lower active aligners and an additional 2.3 mm of IPR between the lower anterior segment.
- Optimized multi-level components on right 6s and UL6
- Optimized root control attachments on UR5 and UL3
- Optimized LR4, LR3 and LL3 rotation component
- Optimized UR4, UL4 and LL5 retention attachments
- 5mm U6s and UL5 horizontal bevel fittings
- 4mm horizontal beveled components on the palatal surface of U1s and U2s
- L6s horizontal occlusal bevel attachments.
An additional six upper and lower active aligners were needed to close the remaining spaces and correct the bite.
Conservation protocol
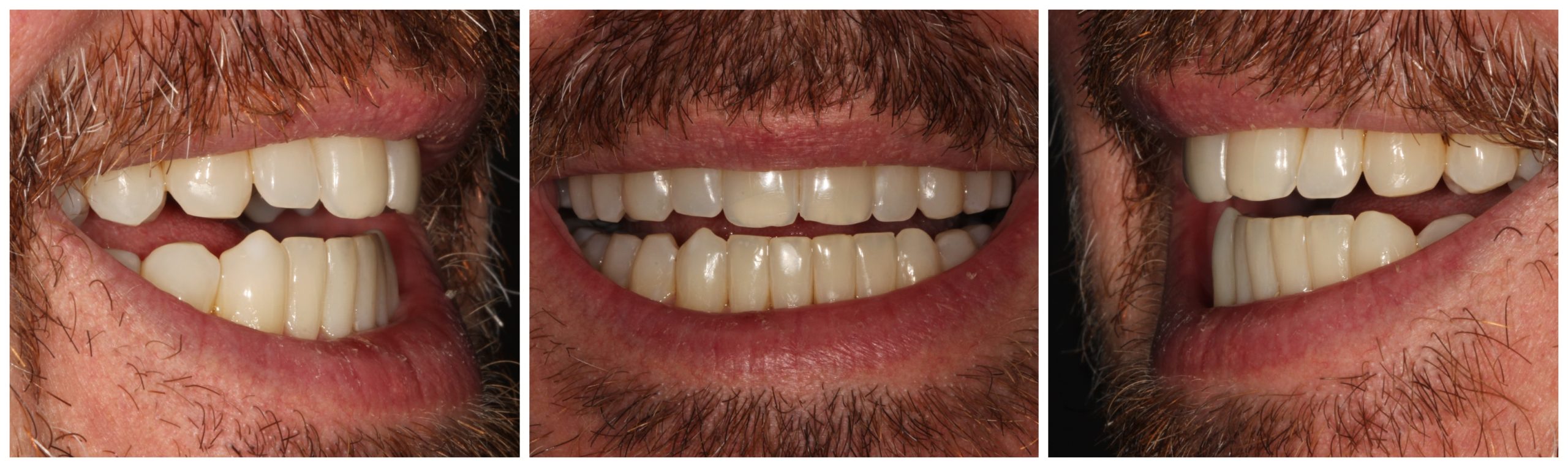
At this point we discussed chipped U1s and discussed butt welding. The patient was not interested in reshaping his teeth as he liked them still looking like his own teeth.
Vivera retainers were fitted to be worn 20-22 hours a day for eight weeks. After that the patient had to use them only at night. The patient was aware of the need for indefinite retention to minimize both recurrence and maturational changes.
The patient is very happy with the results and decided to put the cherry on the teeth whitening cake. We used Enlighten Smiles teeth whitening.

If you want to become confident in treating this type of treatments, you need to learn the basics well. My Diamond Masterclass aims to discuss every aspect of Invisalign in a friendly and straightforward manner, including:
- Consultation
- Records and Orthodontic Evaluation
- Biomechanics
- Click on modifications and 3D controls
- Attachments
- IPR.
The next Diamond Masterclass is on March 2, 2024.
For more information visit www.alignertraining.com.